Utilizing Fiberoptic Endoscopic Evaluation of Swallowing (FEES®) with the Passy Muir Valve to Facilitate Successful Decannulation
This content is sponsored by Passy-Muir
Decannulation, the removal of a tracheostomy tube, is a significant milestone in the care of patients with tracheostomies (Christiansen et al., 2022). It represents the restoration of a more natural airway and signifies improved respiratory function. However, correlations between swallowing and decannulation have been investigated. Escudero et al. (2022) found that poor swallowing function was negatively associated with successful decannulation. Therefore, decannulation often involves careful assessment and management of swallowing function to ensure safety and successful transition to oral feeding while also addressing decannulation (Escudero et al., 2022). In patients with tracheostomy, the additional issue of having an open system with reduced pressures and decreased use of the upper airway further complicates the decannulation process. Using a Passy Muir® Tracheostomy & Ventilator Swallowing and Speaking Valve (PMV®) to close the system also has been shown to assist with decannulation (Zhou et al., 2022, O’Connor et al., 2019). By combining these two techniques, FEES and PMV use, healthcare professionals can effectively evaluate and manage swallowing function, while facilitating safe and successful decannulation.
Understanding FEES
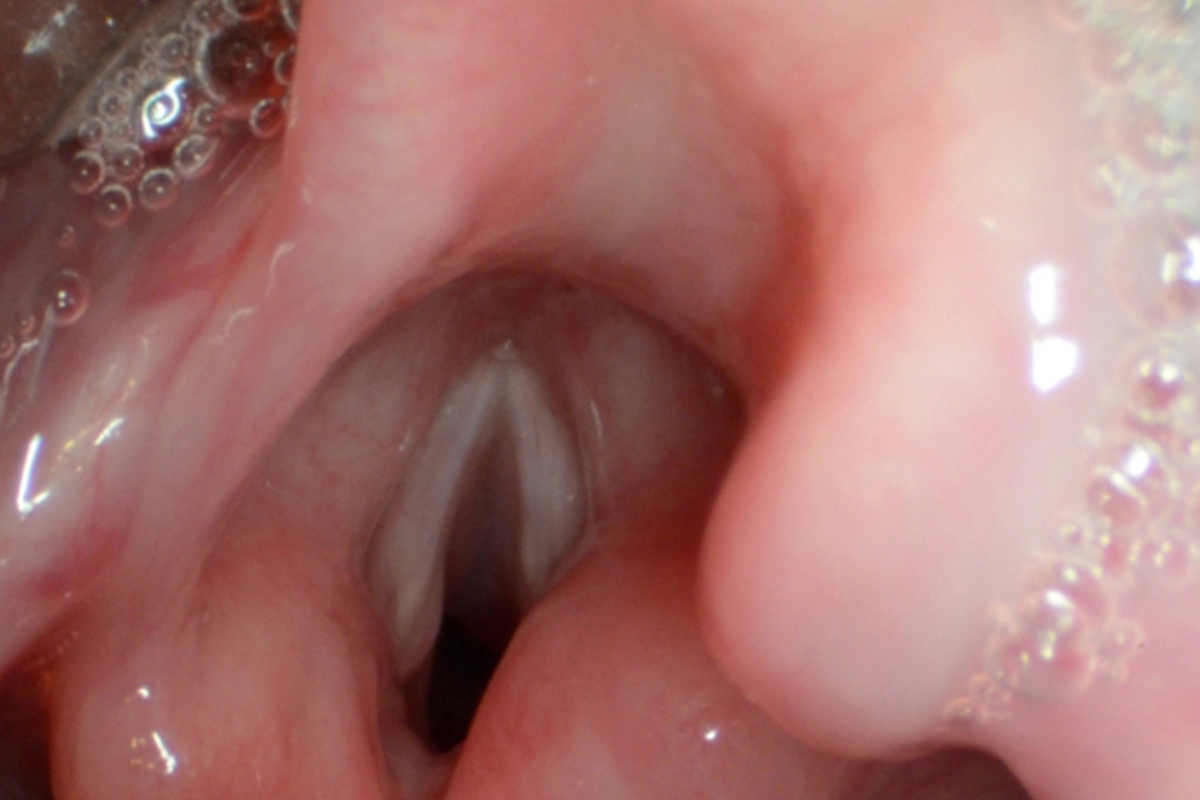
Fiberoptic Endoscopic Evaluation of Swallowing (FEES) is a procedure that utilizes a flexible endoscope to visualize the pharynx and larynx during swallowing. During FEES, the endoscope is passed through the nasal cavity to the pharynx, providing real-time visualization of the swallowing process. This procedure allows for the assessment of anatomical and physiological aspects of swallowing, including timing, coordination, and presence of aspiration or penetration. During a FEES assessment, it also is possible for the clinician to view secretions in the upper airway and supraglottic region, along with viewing the state of the vocal folds (Starmer, 2022).
Benefits of Combining FEES and the Passy Muir Valve
- Objective Assessment of Swallowing Function: FEES allows healthcare professionals to directly observe the swallowing process, providing valuable information about the safety and efficiency of swallowing. By incorporating the Passy Muir Valve (PMV) during FEES, clinicians can assess the impact of the valve on swallowing function and make informed decisions regarding decannulation readiness.
- Identifying Aspiration and Penetration: FEES enables the detection of aspiration and penetration, which are significant concerns during decannulation. During FEES, the clinician may assess how this reduces aspiration or penetration events. This combined approach allows clinicians to make evidence-based decisions regarding decannulation safety (Escudero et al., 2022).
- Assessing Airway Protection: The Passy Muir Valve supports airway protection during swallowing by facilitating glottic closure. The Valve restores more functional cough and throat clear through use of the upper airway and restored pressures (O’Connor et al., 2019). FEES can help assess the effectiveness of the Valve in preventing material from entering the airway during swallowing, ensuring a more safe (protected airway) oral intake.
- Determining Timing and Coordination: FEES with the Passy Muir Valve provides insights into the timing and coordination of swallowing. It allows clinicians to evaluate the impact of the valve on the respiratory-swallowing coordination and ensure that the patient can maintain an appropriate breathing pattern during oral feeding (Han et al., 2022).
- Gradual Transition to Oral Feeding: The Passy Muir Valve can be used during FEES to assess the patient’s tolerance and readiness for oral feeding. Use of the Valve during swallowing trials as part of the assessment process allows clinicians to observe the impact on swallowing function and determine if the patient can safely tolerate oral feeds. It also assists with identifying if use of the Valve during oral feeding may be necessary for protection of the airway.

Clinical Considerations and Protocol
- Collaboration and Multidisciplinary Approach: Successful decannulation and management of swallowing function require collaboration among healthcare professionals, including otolaryngologists, speech-language pathologists, respiratory therapists, and nurses (Mah et al., 2017). Each team member contributes their expertise to ensure comprehensive evaluation and management.
- Patient Selection: Careful patient selection is crucial when considering decannulation and utilizing FEES with the Passy Muir Valve. Ideally, candidates should demonstrate stable respiratory status, appropriate cognitive function, and adequate swallowing abilities to ensure safety during the decannulation process. However, some patients may be decannulated who still demonstrate reduced functions.
- Step-wise Evaluation: The decannulation process should be approached step-by-step. Considering that the patient’s respiratory and swallowing function are impacted by an open tracheostomy tube, the first place to start is closing the system. This would entail using the Passy Muir Valve to redirect airflow up to the mouth and nose and reengaging the upper airway function. With a closed system, swallowing can then be addressed as the airflow and pressures have been redirected into a more normal pattern. Swallowing assessment, including instrumental assessment with FEES, may be performed at different stages to assess swallowing function with and without the valve, ensuring that the patient can safely tolerate oral feeds. Some patients may not be able to use a speaking valve and then that step may be bypassed. However, if unable to tolerate a Passy Muir Valve, this may be an indication of issues that would negatively impact decannulation (Escudero et al., 2022).
- Objective Assessment Criteria: Specific criteria should be established to determine decannulation readiness based on the FEES findings, Valve use, and patient’s medical status. These criteria may include absence of aspiration or penetration, effective airway protection, appropriate timing and coordination, and safe oral intake with the Passy Muir Valve.
- Monitoring and Follow-up: Close monitoring and frequent follow-up are essential throughout the decannulation process. Post-decannulation, assessment of swallowing function should be conducted to ensure long-term safety and successful transition to oral feeding.
Benefits and Impact on Patients
The utilization of FEES with the Passy Muir Valve during the decannulation process offers several benefits for patients:
- Enhanced Safety: The combined approach allows clinicians to objectively evaluate swallowing function and make informed decisions regarding decannulation, ensuring the patient’s safety during oral feeding.
- Improved Swallowing Function: The Passy Muir Valve supports effective airway protection and promotes optimal swallowing function (Han et al., 2022; O’Connor et al., 2021; O’Connor et al., 2019). By using FEES, clinicians can assess the valve’s impact on swallowing and adjust management strategies accordingly.
- Psychological and Quality of Life Benefits: Successful decannulation enhances the patient’s self-esteem, independence, and overall quality of life. The use of FEES with the Passy Muir Valve provides a comprehensive approach that focuses on patients’ long-term well-being and functional outcomes (Freeman-Sanderson et al., 2018).
Conclusion
The combination of FEES with the Passy Muir Valve offers a comprehensive and evidence-based approach to facilitate safe and successful decannulation. By objectively evaluating swallowing function, identifying aspiration risks, and determining the impact of the Passy Muir Valve on swallowing dynamics and respiratory function, healthcare professionals can make informed decisions regarding decannulation readiness. This approach ensures patient safety, promotes optimal swallowing function, and enhances the patient’s overall quality of life post-decannulation. The utilization of FEES with the Passy Muir Valve represents a valuable tool in the management of patients undergoing decannulation, supporting successful transition to safe and effective oral feeding.
References
Christiansen, K. J., Devantier, L., Pasgaard, T., Benson, T. E., Petersen, J. J., Kjærgaard, T., & Pedersen, M. (2022). Tracheostomy healing time after decannulation. Multidisciplinary Respiratory Medicine, 16(1), 822. https://doi.org/10.4081/mrm.2022.822
Escudero, C., Sassi, F. C., de Medeiros, G. C., de Lima, M. S., Cardoso, P. F. G., & de Andrade, C. R. F. (2022). Decannulation: a retrospective cohort study of clinical and swallowing indicators of success. Clinics (Sao Paulo, Brazil), 77, 100071. https://doi.org/10.1016/j.clinsp.2022.100071
Freeman-Sanderson, A. L., Togher, L., Elkins, M., & Kenny, B. (2018). Quality of life improves for tracheostomy patients with return of voice: A mixed methods evaluation of the patient experience across the care continuum. Intensive & Critical Care Nursing, 46, 10–16. https://doi.org/10.1016/j.iccn.2018.02.004
Han, X., Ye, Q., Meng, Z., Pan, D., Wei, X., Wen, H., & Dou, Z. (2022). Biomechanical mechanism of reduced aspiration by the Passy-Muir valve in tracheostomized patients following acquired brain injury: Evidences from subglottic pressure. Frontiers in Neuroscience, 16, 1 – 13. https://doi.org/10.3389/fnins.2022.1004013
Mah, J. W., Staff, I. I., Fisher, S. R., & Butler, K. L. (2017). Improving decannulation and swallowing function: A comprehensive, multidisciplinary approach to post-tracheostomy care. Respiratory Care, 62(2), 137–143. https://doi.org/10.4187/respcare.04878
O’Connor, L. R., Morris, N. R., & Paratz, J. (2019). Physiological and clinical outcomes associated with use of one-way speaking valves on tracheostomised patients: A systematic review. Heart & Lung, 48(4), 356-364. https://doi.org/10.1016/j.hrtlng.2018.11.006
O’Connor, L. R., Morris, N., & Paratz, J. (2021). The safety and efficacy of prolonged use of one-way speaking valves. Australian Critical Care, 34(4), 319-326. https://doi.org/10.1016/j.aucc.2020.09.003
Starmer, H. M. (2022). Incorporating Flexible Endoscopic Evaluation of Swallowing Rating Scales Into Clinical Practice. Perspectives of the ASHA Special Interest Groups, 1-7.
Zhou, T., Wang, J., Zhang, C., Zhang, B., Guo, H., Yang, B., Li, Q., Ge, J., Li, Y., Niu, G., Gao, H., & Jiang, H. (2022). Tracheostomy decannulation protocol in patients with prolonged tracheostomy referred to a rehabilitation hospital: a prospective cohort study. Journal of Intensive Care, 10, 34, 1 – 9. https://doi.org/10.1186/s40560-022-00626-3

