
Introduction: A Torch Rekindled
In September of 2019, I gave a talk for the University of Florida’s Medical SLP Grand Rounds series with the cute, cheeky title: “Relationship Status: It’s Complicated. The SLP and Aspiration Pneumonia”. I had been inspired by recent literature on the diagnosis of aspiration pneumonia and was going through the start of an existential crisis. If much of what SLPs do in clinical practice stems from a perceived need to protect patients from a potentially-fatal lung infection, but the evidence behind that underlying rationale is dicey, could there be trouble? I mean, that had been a huge motivation of mine when working in skilled nursing facilities in northeast Georgia.
The conversation at that September meeting consisted largely of questions, not answers. A similar tone was struck in Ed Bice and Angela Van Sickle’s Dysphagia Cafe article “Aspiration Pneumonia: the more we learn the less we know,” from September 2020 (I will henceforth reference this as “The Less We Know”). Mr. Bice and Dr. Van Sickle covered a wide range of relevant topics and referenced an impressive sixty-six academic sources that guide and ground their writing, with The Less We Know garnering over 22,000 views (as of June, 2021). If you have not read it yet, you may wish to start there. After reading it, I felt like it was time to update my talk from September 2019 and further develop my thoughts on the topic of aspiration pneumonia as it relates to SLP clinical practice. My approach to the topic differs as I am a doctoral student who has not worked clinically since 2016, though I hope this will not induce SLPs to dismiss my take as irrelevant or off-base. It is my intention to help, building on others’ contributions, from the perspective of somebody who has the luxury to access and evaluate the literature (i.e., dig into Rabbit Holes).
The Proliferation of Aspiration Pneumonia in Dysphagia Literature…Where did it Begin?
In 1998, the journal Dysphagia published the massively impactful article by Susan Langmore and colleagues, “Predictors of Aspiration Pneumonia: How Important is Dysphagia?” SpringerLink shows over 500 citations, while GoogleScholar shows that this paper has been cited over 1000 times. Here are just a few quotes citing Langmore et al., 1998, demonstrating how this paper has been referenced:
“The relationship between laryngeal aspiration and pneumonia has been well recognized (Langmore et al., 1998).” Ashford, 2005
“Accurate identification of individuals who are at risk for oropharyngeal dysphagia is critically important because of the high incidence of pneumonia associated with unrecognized prandial aspiration (Langmore et al., 1998 and 3 other citations)” Suiter & Leder, 2008
“Feeding dependence poses an increased risk for aspiration and related complications in patients with dysphagia due to factors such as rapid and uncontrolled presentation of food by feeders (Langmore et al., 1998)” Sura et al., 2012
“Dependency upon others for feeding or oral care and number of decayed teeth were best predictors for aspiration pneumonia (Langmore et al., 1998).” Sjogren et al., 2008
Whenever I re-read this paper, I feel inspired to do strong, well-designed research. No wonder it has become such a pillar in our evidence base. It details a four-year prospective study of elderly Veteran’s Administration patients that included videofluoroscopic swallow studies, fiberoptic endoscopic evaluations of swallowing (FEES; in half of subjects), detailed oral examinations, as well as annual functional and physical metrics (Langmore et al., 1998). Using these longitudinal data, the researchers looked back at factors that preceded and presumably contributed to the development of pneumonia. Despite all its methodological strengths, as a trainee in pursuit of a career as a researcher in dysphagia, there are points I would like to raise for consideration. To approach these issues, we’ll dip our toes into some terminology; before you know it, we’ll be fully submerged.
Gold or Pyrite?
Many readers are familiar with the term “operational definition”, which indicates how a word or phrase is to be used in the context of a research study or publication. It helps the author to be clear, and for the reader to know what is included and excluded by the term. For example, articles in our field often reference “dysphagia” while operationally defining it as oropharyngeal dysphagia, excluding esophageal issues. Operational definitions are critical especially when referencing terms that can be used differently by various people, professions, etc., as often happens in medicine. It gives me pause to notice the lack of an operational definition of aspiration pneumonia in an article seeking to explain predictors or risk factors of that very condition (i.e., Langmore et al., 1998). The terms “pneumonia” and “aspiration pneumonia” are used interchangeably throughout the text. The reader could assume that any time they read “pneumonia” in this article, they can infer that it means “aspiration pneumonia”, especially if they find reassurance in the methods section. The methods detail diagnostic criteria for a diagnosis of pneumonia, including expert panel agreement on (1) elevated white blood cell count, (2) fever, and (3) findings on a chest radiograph, plus (4) exclusion of “nonaspiration-related pneumonia, such as hematogenous [i.e., spread via blood] pneumonia” (Langmore et al., 1998). I looked into what other non-aspiration options might have been and found some clarity: “inhalation of infectious aerosols [or] spread of infections from contiguous sites,” (Azarpazhooh & Leake, 2006). An explanation about how the expert panel differentiated between “aspiration pneumonia” and “nonaspiration-related pneumonia” is absent (Langmore et al., 1998).
Personally unconvinced, I found further evidence for my uncertainty in more recent literature. For instance, aspiration pneumonia has been called out as having a “lack of sufficient diagnostic criteria to be considered a distinct clinical diagnosis” (Ferguson et al., 2018). Indeed, “robust diagnostic criteria for aspiration pneumonia are lacking” (Mandell & Niederman, 2019). These representative excerpts seem to explain, if not excuse, the ambiguity present in 1998. I do not mean to suggest this lack (and perhaps impossibility) of an operational definition for aspiration pneumonia is a “fatal flaw”, nor that I am the first person to notice that this murkiness can be problematic (Jurado & Franco-Paredes, 2001). What I mean to express is my view that research establishing facts about a specific diagnosis (i.e., aspiration pneumonia) should start with a gold standard evaluation to ensure the diagnosis itself is valid. In the case of aspiration pneumonia, that type of gold standard does not exist (Hollaar et al., 2016; Ferguson et al., 2018; Mandell & Niederman, 2019; Lindenauer et al., 2018, Gon Son et al., 2017). Further, the argument has been made that the term is so misleading, it ought to be dismissed (Jurado & Franco-Paredes, 2001; Ferguson et al., 2018; Mandell & Niederman, 2019). From all that I have seen, our field has not yet come to any such consensus on the phrase.
Questions, Rabbit Holes, and Swallowing Converge
However, if an individual SLP accepts concerns about the term as valid, how is decades of research on “aspiration pneumonia” to be interpreted? If one trusts these experts (e.g., Ferguson et al., 2018; Mandell & Niederman, 2019; Jurado & Franco-Parades, 2001), yet continues to cite work about the incidence of aspiration pneumonia, won’t this ambiguity and outright confusion persist? Confusion is pretty common (in my opinion) when you pursue a PhD or seek to become an expert in any given academic or medical area–the more you look, the more questions you find (e.g., “The Less We Know”). Still, I try to answer the questions that persistently bounce about my brain: “Was there formerly a gold standard to identify aspiration pneumonia? That would explain much of the previous research I’m concerned about. If not, are SLPs’ efforts in pneumonia prevention via dysphagia management anything like what I believed? The risk of pneumonia kept me convinced of the critical importance of my clinical practice when I worked previously…could my reasoning have been misguided?”
This kind of thinking is what leads me down Rabbit Holes. You know, the kind of Internet sleuthing deep-dive that leads you to lose track of time and to feel rather dizzy. To begin my descent, my process is to find an impactful statement in one publication and look at the citation. Then I find the reference and identify the source text (i.e., when the article was cited, which part of the text was being referenced?). Next I look at that reference (often thanks to the glory of the Interlibrary Loan (ILL) system) and on and on to locate the earliest reported findings I can identify. It can take what feels like forever, but it’s a worthwhile pursuit. Why? It’s like breaking apart the game Telephone, where successive whisperings of a message from person to person change the telling. Sometimes the differences from publication to publication are subtle…sometimes they are stark. I’m going to walk you through how I do this, using a relevant example from The Less We Know. I hope it will show you how and why I bother with these Rabbit Holes in the first place, given the significance of this topic in our field.
Back Above Ground: What Have We Unearthed?
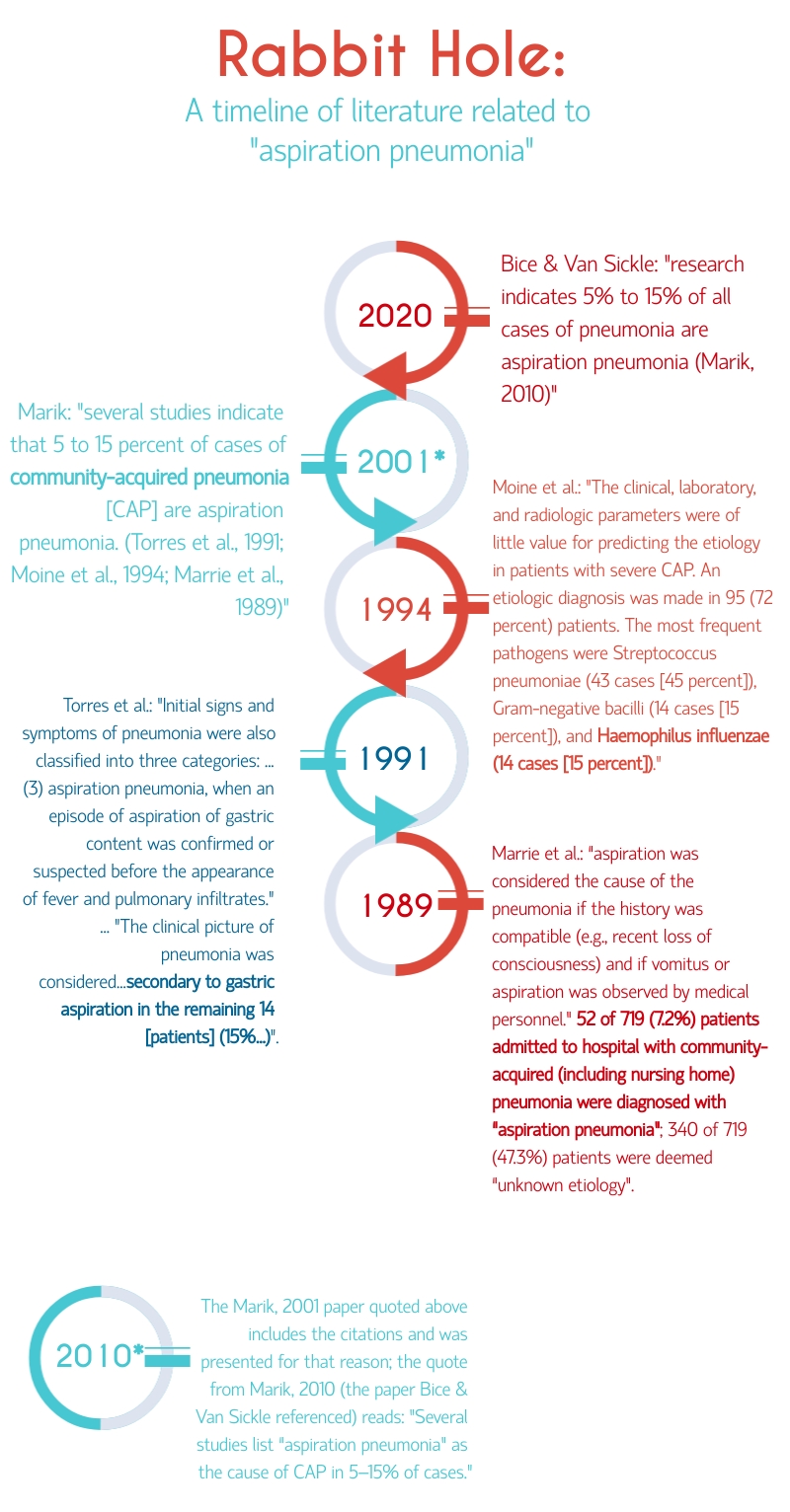
Not all that glitters is gold. By descending into the literature and reemerging with just a few pieces of evidence, we can see some important distinctions between recent summaries about aspiration pneumonia and early reports. For instance, early work looked at “aspiration pneumonia” among hospitalized patients who had severe community-acquired pneumonia (Torres et al., 1991; Marrie et al., 1989). Differences in findings may have been due to varying methodological factors, from diagnostic criteria (i.e., what constituted “aspiration pneumonia”) to the characteristics of the population (i.e., age, underlying conditions, living situation). While these studies often employed invasive techniques to identify the infectious agent in diagnosed pneumonia (Torres et al., 1991; Moine et al., 1994; Marrie et al., 1989), none included any instrumental assessments of dysphagia (e.g., videofluoroscopy, FEES) that Langmore and colleagues used. Indeed, the identification of aspiration in earlier literature is often based on clinical observation or history consistent with gastric aspiration (Torres et al., 1991; Marrie et al., 1989). Beyond this, one study did not mention the route of infection (i.e., aspiration) at all, instead only describing the infectious bacteria (i.e., Haemophilus influenzae; Moine et al., 1994). This bacteria can be presumed to come from the nose and mouth (Japanese Respiratory Society, 2009), implying that it emigrated to the lungs via aspiration. Since we understand that aspiration can happen regularly in healthy adults during sleep (Gleeson et al., 1997), how convinced are you that the presence of certain bacteria in the lungs is the result of dysphagia-related aspiration? Would you feel comfortable making this inference in the context of a research study that will be disseminated to SLPs all over the world to impact their clinical practice?
Similar and Different All At Once: The Less We Know
The Less We Know stated that aspiration pneumonia is a “vague diagnosis”, citing some of the same authors I referenced who would prefer to abandon the term. Bice and Van Sickle also point out the lack of a gold standard diagnostic tool for aspiration pneumonia, as well as the complex mechanism for the development of pneumonia, wherein aspiration is insufficient on its own to cause a lung infection. I enjoyed their discussion about the microbiome of the lungs and oral cavity as well as the function of the mucociliary escalator that helps remove potentially infectious agents from the airway. Despite these gems, I remain skeptical of any sentence that uses phrases like “all” or “none”, even when backed up by a citation (the quote of theirs I went into the Rabbit Hole for). I know we don’t always have time to dive back into the literature when we see claims or interpretations that cause our brows to raise. To be more fair and realistic, we probably often don’t have time for that, nor do I have a solution for this conundrum. I do have some different opinions than Bice and Van Sickle, based upon my personal interpretations.
It’s Fine to Opine:
- No, stopping aspiration “at all costs” should definitely not be the goal of swallowing therapy. In brief, this does not appear to be based in evidence, nor (in the current literature) is aspiration on its own enough to cause pneumonia. Evidence-based practice still requires us to incorporate the needs and values of our clients and their families, who presumably have multifaceted and nuanced goals for swallowing therapy (e.g., quality of life, nutrition, satiety) that deserve respect and consideration.
- No, a chest x-ray can not accurately provide a diagnosis of “aspiration pneumonia”–nothing can. Again, there is currently no gold standard for this diagnosis.
Concluding Advice from the Spelunker in Training
Given my hot takes, I’ll offer some general unsolicited advice to practicing SLPs following a brief disclaimer. This website is a phenomenal resource – I was the one who asked Jonathan Waller if I could submit this post for consideration. That said, we know not all publications are vetted equally. When looking into the evidence on any topic, remember these general guidelines.
- The presence of a bunch of citations does not necessarily mean all the information presented is an accurate representation of the referenced material, and I’m not just talking about blogs. There has been a proliferation of journals that practice “Predatory Publishing”, following a pay to publish model. Pro tip: you can actually look and see the time gap between receipt of a manuscript and the acceptance and/or publication date…if it’s suspiciously short, be suspicious of the peer review process.
- Next, in any publication, beware of terms like “all” or “none”. Remember the tips you learned for taking standardized tests like the ACT, SAT, or GRE? We generally understand that most things seem to have more nuance rather than absolutes, particularly in dysphagia management and speech-language pathology more broadly.
- My last tip is to simply do your best. In the absence of compelling evidence from research literature, you must rely on your experience, clinical judgements, and the needs and preferences of your patients and their loved ones. That’s what evidence-based practice is all about.
I do not believe we should reject or ignore the literature on pneumonia just because the terminology is a mess. Instead, I see options. One option is to do a mental Find & Replace on the literature, replacing all instances of “aspiration pneumonia” simply with “pneumonia”. Another option would be to limit our attention to literature that is meant for us as SLPs. If we focus on studies that confirmed the presence of dysphagia and followed participants longitudinally, we may be more convinced of outcomes relating to the development of pneumonia. Another more dramatic choice is to grab our favorite red pens, read all the literature as before, but emphatically underline and write angry notes in the margins (been there, done that) each time we see the words “aspiration pneumonia”. Lastly, perhaps there is an argument to be made for coining a new term…”dysphagic pneumonia?” I’m certainly getting ahead of myself with that idea, but I hope you will contemplate your own practice and how you’ll think about these terms and concepts in the future.
If you ever dive down any interesting Rabbit Holes related to this topic, I am always interested in chatting! Please feel free to reach out and thank you so much to Jonathan for allowing me to present these thoughts. Thank you also to Ed Bice and Dr. Van Sickle for reigniting the torch I’ll always carry for “aspiration pneumonia”.
The full contents of this article solely represent the ideas and opinions of Ms. Rivet and do not necessarily represent the views of the University or Dr. Hegland.
References
References:
Ashford John R. (2005). Pneumonia: Factors Beyond Aspiration. Perspectives on Swallowing and Swallowing Disorders (Dysphagia), 14(1), 10–16. https://doi.org/10.1044/sasd14.1.10
Azarpazhooh, A., & Leake, J. L. (2006). Systematic review of the association between respiratory diseases and oral health. Journal of periodontology, 77(9), 1465–1482. https://doi.org/10.1902/jop.2006.060010
Ferguson, J., Ravert, B., & Gailey, M. (2018). Aspiration: Noun: An ambiguous term used for a diagnosis of uncertainty. Clinical Pulmonary Medicine, 25, 177-183.
Gleeson, K., Eggli, D. F., & Maxwell, S. L. (1997). Quantitative aspiration during sleep in normal subjects. Chest, 111(5), 1266–1272. https://doi.org/10.1378/chest.111.5.1266
Hollaar, V., van der Maarel-Wierink, C., van der Putten, G. J., van der Sanden, W., de Swart, B., & de Baat, C. (2016). Defining characteristics and risk indicators for diagnosing nursing home-acquired pneumonia and aspiration pneumonia in nursing home residents, using the electronically-modified Delphi Method. BMC geriatrics, 16, 60. https://doi.org/10.1186/s12877-016-0231-4
Japanese Respiratory Society (2009). Aspiration pneumonia. Respirology (Carlton, Vic.), 14 Suppl 2, S59–S64. https://doi.org/10.1111/j.1440-1843.2009.01578.x
Jurado, R. L., & Franco-Paredes, C. (2001). Aspiration pneumonia: a misnomer. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 33(9), 1612–1613. https://doi.org/10.1086/323016
Langmore, S. E., Terpenning, M. S., Schork, A., Chen, Y., Murray, J. T., Lopatin, D., & Loesche, W. J. (1998). Predictors of aspiration pneumonia: how important is dysphagia?. Dysphagia, 13(2), 69–81. https://doi.org/10.1007/PL00009559
Lindenauer, P. K., Strait, K. M., Grady, J. N., Ngo, C. K., Parisi, M. L., Metersky, M., Ross, J. S., Bernheim, S. M., & Dorsey, K. (2018). Variation in the Diagnosis of Aspiration Pneumonia and Association with Hospital Pneumonia Outcomes. Annals of the American Thoracic Society, 15(5), 562–569. https://doi.org/10.1513/AnnalsATS.201709-728OC
Mandell, L. A., & Niederman, M.S. (2019) Aspiration Pneumonia. N Engl J Med; 380:651-663. DOI: 10.1056/NEJMra1714562
Marik P. E. (2001). Aspiration pneumonitis and aspiration pneumonia. The New England journal of medicine, 344(9), 665–671. https://doi.org/10.1056/NEJM200103013440908
Marik, P. E., & Kaplan, D. (2003). Aspiration pneumonia and dysphagia in the elderly. Chest, 124(1), 328–336. https://doi.org/10.1378/chest.124.1.328
Marrie TJ, Durant H, Yates L. Community-acquired pneumonia requiring hospitalization: 5-year prospective study. Rev Infect Dis 1989;11:586-599
Moine P, Vercken JP, Chevret S, Chastang C, Gajdos P. Severe community-acquired pneumonia: etiology, epidemiology, and prognosis factors. Chest 1994;105:1487-1495
Sjögren, P., Nilsson, E., Forsell, M., Johansson, O. and Hoogstraate, J. (2008), A Systematic Review of the Preventive Effect of Oral Hygiene on Pneumonia and Respiratory Tract Infection in Elderly People in Hospitals and Nursing Homes: Effect Estimates and Methodological Quality of Randomized Controlled Trials. Journal of the American Geriatrics Society, 56: 2124-2130. https://doi.org/10.1111/j.1532-5415.2008.01926.x
Son, Y.G., Shin, J., & Ryu, H.G. (2017). Pneumonitis and pneumonia after aspiration. J Dent Anesth Pain Med, 17(1):1-12
Suiter, D. M., & Leder, S. B. (2008). Clinical Utility of the 3-ounce Water Swallow Test. Dysphagia, 23(3), 244–250. https://doi.org/10.1007/s00455-007-9127-y
Sura, L., Madhavan, A., Carnaby, G., & Crary, M. A. (2012). Dysphagia in the elderly: management and nutritional considerations. Clinical interventions in aging, 7, 287–298. https://doi.org/10.2147/CIA.S23404
A. Torres, J.D. Chalmers, C.S. Dela Cruz, C. Dominedo, M. Kollef, I. Martin-Loeches, …, R.G. Wunderink (2019). Challenges in severe community-acquired pneumonia: a point-of-view review. [Review] Intensive Care Med., 45 (2) (2019), pp. 159-171, 10.1007/s00134-019-05519-y




{kind=link}